
- 1. What are the different phases of normal wound healing?
- 2. What are the main factors involved in delayed wound healing?
- 3. Which medicinal products affect wound healing?
- 4. What is the impact of topical corticosteroids on wound healing?
- 5. Is there a difference between wound healing in acute and chronic wounds?
- 6. How should you clean wounds?
- 7. What are the specific features of wound healing in children?
- 8. What are the specific features of wound healing in the elderly?
- 9. How to manage wound healing in cancer patients?
- 10. What are the specific features of wound healing in patients with burn injuries?
- 11. What dressing should be used according to the appearance of the wound?
- 12. What role do dermocosmetics play in wound healing?
- 13. Is there a role for alternative therapies in wound healing?
- 14. What advice should be given to patients to achieve an optimal scar (postoperative and post-trauma)?
- 15. What is a pathological scar and why does it develop?
- 16. How do you treat pathological scars?
- 17. How do you treat and heal a leg ulcer?
- 18. How do you treat and heal a pressure sore?
- 19. How do you treat and heal a foot wound in a diabetic patient?
- 20. What is the relationship between wound healing and mental health?
15. What is a pathological scar and why does it develop?
Healing as described above represents the physiological model of normal healing. In some cases, however, when healing does not occur normally, this is referred to as a pathological scar which can result from either delayed healing (leading to a chronic wound) or an excess scarring process (Figure 8).
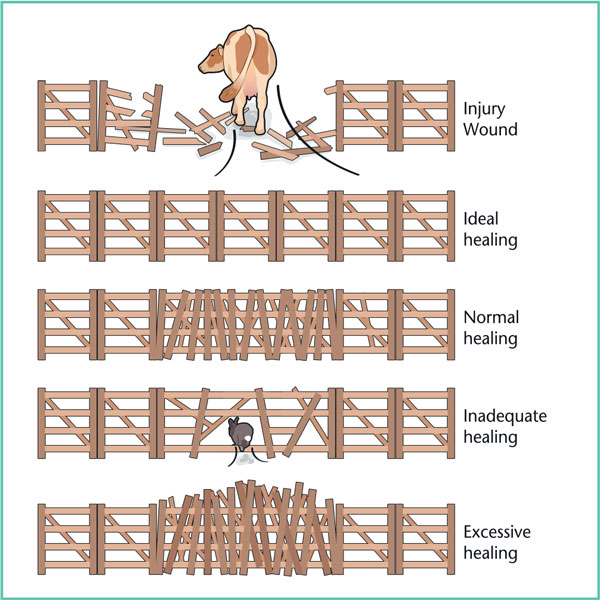
Figure 8. Ideal, insufficient, excessive healing.
There are two clinical forms of pathological scar healing: hypertrophic scars and keloid scars, which have an identical initial phase of healing called hypertrophic. However, their progression differs: simple hypertrophic scars progress favourably over 12-18 months, usually in the form of a larger scar. While keloid scars do not tend to improve spontaneously.
Due to excessive scarring, a hypertrophic scar is thick, erythematous and often pruritic (Figure 9). Unlike keloid scars, however,it is limited to the area of injury and does not extend beyond it.

Figure 9. Hypertrophicscar.
Keloid scars are characterised by excessive activity during wound healing, resulting in thick, hyalinised, disorganised and excessive collagen fibres (Figure 10) [8]. Thus the extracellular matrix is abundant, while cellularity is low. The appearance is described as being like “crab claws”, extending beyond the initial scar bed unlike hypertrophic scars.
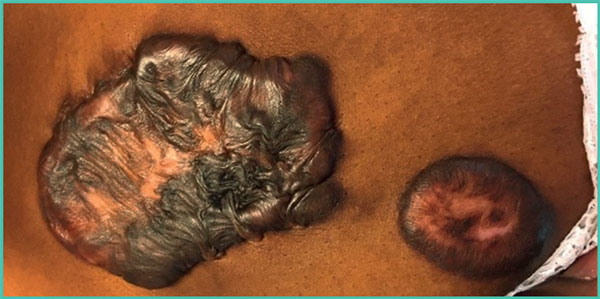
Figure 10. Keloid scars.
We still do not really understand the mechanism that causes keloid scarring. Several hypotheses have been suggested such as prolonged activation of the proliferative phase of fibroblasts, decreased apoptosis, an increase in metalloproteinase inhibitors and lower collagenase activity.
Several risk factors for the occurrence of these scars have been identified such as having a dark skin type, hormonal factors (occurs more frequently during pregnancy and puberty), orientation of the wound in relation to skin tension lines and location of the wound (Figure 11).
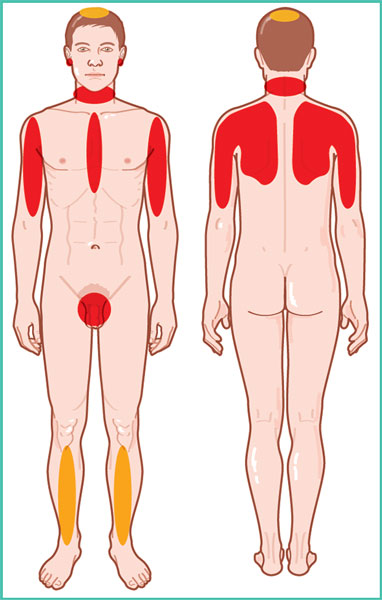
Figure 11. Location of keloid scars.Fre- quent in red and rare in yellow.
References
1. Singer AJ, Clark RA. Cutaneous wound healing. N Engl J Med 1999;341: 738-46.
2. Eming SA, Krieg T, Davidson JM. Inflammation in wound repair: molecular and cellular mechanisms. J Invest Dermatol2007; 127: 514-25.
3. Suivi en ville des plaies chroniques : ulcère veineux de jambe, escarre, plaie du pied diabétique. Assurance maladie, octobre 2015.
4. Plaies aiguës en structure d’urgence. Référentiel de bonnes pratiques. SFMU, 2017: 32 p.
5. Sgonc R, Gruber J. Age-related aspects of cutaneous wound hea- ling: a mini-review. Gerontology 2013; 59: 159-64.
6. Majtan J. Honey: an immunomodulator in wound healing. Wound Repair Regen 2014; 22: 187-92.
7. Opletalová K, BlaizotX, Mourgeon B, et al. Maggot therapyfor wound debridement: a randomized multicenter trial. Arch Dermatol 2012; 148: 432-8.
8. van den Broek LJ, Limandjaja GC, Niessen FB, Gibbs S. Human hypertrophic and keloid scar models: principles, limitations and future challenges from a tissueengineering perspective. ExpDer- matol 2014; 23: 382-6.
9. Prise en charge de l’ulcère de jambe à prédominance veineuse hors pansement. Recommandations HAS, 2006.
10. La compression médicale dans les affections veineuses chroniques. Fiche de bon usage HAS, 2010.
11. Edmonds M, Lázaro-Martínez JL, Alfayate-García JM, et al. Sucrose octasulfate dressing versus control dressing in patients with neu- roischaemic diabetic foot ulcers (Explorer): an international, multi- centre, double-blind, randomised, controlled trial [published correction appears in Lancet Diabetes Endocrinol 2018]. Lancet Diabetes Endocrinol 2018; 6: 186-96.
12. Reinholz M, Poetschke J, Schwaiger H, Epple A, Ruzicka T, Gauglitz GG. The dermatology life quality index as a means to assess life quality in patients with different scar types. J Eur Acad Dermatol Venereol 2015; 29: 2112-9.
With the institutional support of the laboratories